Why Do Anonymous Online Communities Outlast In-Person Treatment?
Tuesday, 10 PM. You stop in front of an ATM at a 24-hour convenience store. Balance: $80. Payday is ten days away.
You saw your therapist Monday afternoon. “Use the breathing technique when the urge hits,” they said. But right now, you can’t quite remember the technique.
Next session is Friday at 2 PM. Three days away.
Relapse in addiction recovery often happens in moments like this. In the gap between treatment sessions.

What’s most fragile is the gap between sessions
Outpatient counseling is typically once a week, 50 minutes. The rest of the week, the person is on their own.
There’s an old saying among addiction self-help groups: “The most dangerous time is between meetings.” It’s a folk truth from members, but the relapse research lines up with it. Most relapses don’t happen during sessions. They happen in the gaps.
Anonymous online communities, available 24/7, come up in this context because of the size of those gaps. In front of an ATM, alone at home at midnight, on a Sunday afternoon. Someone in the same category is there. You can write.
Research on continuation and relapse rates is starting to accumulate. The general direction is settled: combining digital support with in-person treatment yields better results than in-person alone. The disagreement starts after that. What is it that creates the staying-power? And what’s the difference between “lasting” and “working”? The experts haven’t reached consensus.
What people typically point to
A few factors come up consistently as reasons online communities outlast in-person treatment.
The first is time accessibility. Outpatient appointments and in-person meetings are scheduled. Communities are always open. The gap between when an urge hits and when support is reachable is minimized.
The second is anonymity. Addiction is one of the most shame-laden conditions, and “I’m a gambling addict” is often something a person can’t say to family, doctor, or friend first. Social psychology has long known that anonymous online interaction enables faster and deeper self-disclosure than in-person interaction. This is called the online disinhibition effect.
The third is peer presence. Watching someone else with the same condition write daily makes “I’m not alone” land. When recovered people are in the same space, they become a model for what’s possible.
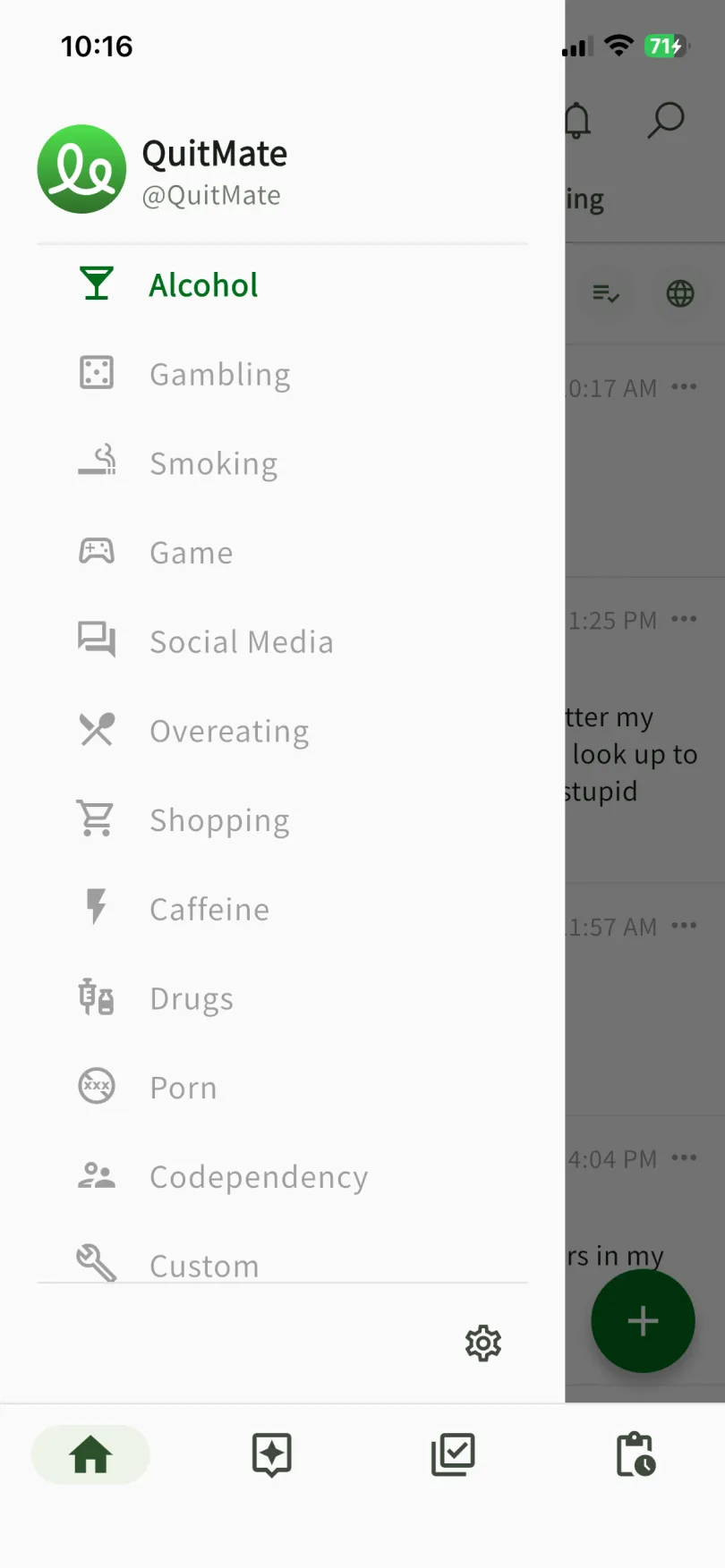
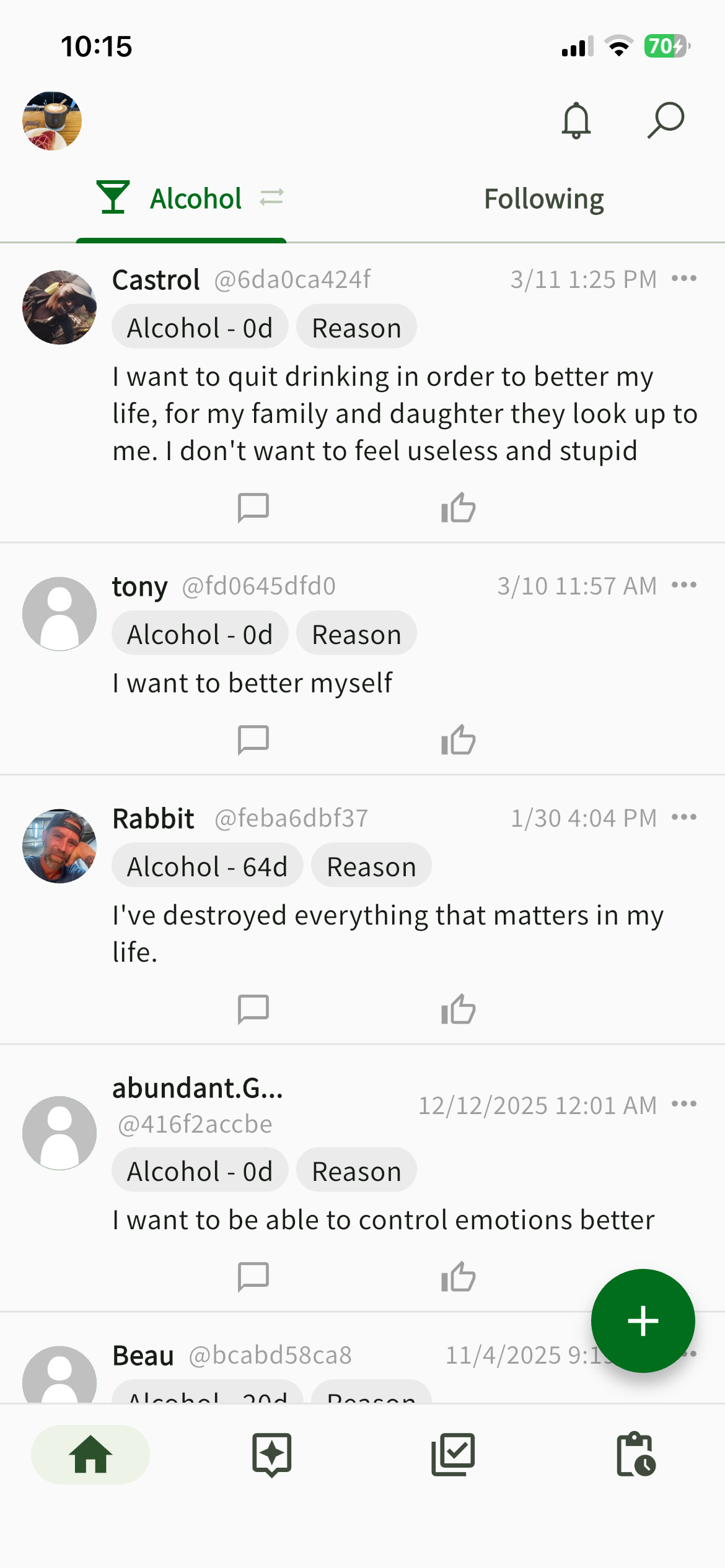
These don’t simply work on their own; design choices change a lot. QuitMate’s internal data, for example, shows a higher write-rate than typical online communities. About 40% of 599 active users have written comments on other people’s posts (details here). The number who post their own status is higher still. The reading-dominant distribution typical of social media (the so-called “90-9-1 rule”) doesn’t apply here. Anonymous handles, a feed showing only people in the same addiction category, posting flow integrated with the day counter, a space focused only on the addiction conversation. Several choices that lower the barrier to writing add up.
”Lasting” and “working” aren’t the same thing
But continuing isn’t the same as recovering.
The U.S. FDA approved reSET-O, a prescription digital therapeutic for opioid use disorder, in 2018. Subsequent research found that reSET-O raises treatment retention to 82.4%, while not reducing substance use any more than standard treatment.
Some experts pushed back on the approval. “Can something that doesn’t reduce symptoms be called treatment?” The FDA has held its position: improvement in retention is itself a meaningful clinical outcome.
The same question gets pointed at online self-help communities. They’re not curing the diagnosis. They don’t reliably reduce symptoms. But they do support the person in staying with treatment or behavioral change. Is that treatment, or the doorway before treatment? There’s no settled answer.
AA has been carrying the same problem for 90 years
The original anonymous addiction community is AA (Alcoholics Anonymous), started in 1935.
A 2020 Cochrane review of AA and 12-step programs analyzed 27 studies covering 10,565 people and concluded that AA outperforms other interventions on sustained sobriety rates. This was received as a major finding in addiction treatment research.
But methodologists have continued to push back. People who keep going to AA tend to be highly motivated to begin with — selection bias. Whether “it works because they keep going” or “they keep going because the people who can keep going show effects” hasn’t been cleanly separated.
That said, no one disputes that the observed effect exists. The argument has stalled at “what’s the active ingredient” and “how does it compare on a level playing field.” Anonymity, peer structure, sustained participation, multiple factors are tangled together, and which one is doing the work is still unsettled.
The 4x gap (median streak by comment count) observed in QuitMate carries the same structural problem. People who write may be more motivated to begin with.
And yet, something is happening
None of these arguments has reached a resting place. The reasons people stick with online communities don’t reduce to a single answer. Whether “lasting” is the same as “working” isn’t settled either.
Even so, one observation is clear: combination matters. A 2025 meta-analysis published in Addiction combined 34 randomized clinical trials (6,461 participants) and found that adding digital support to in-person treatment reduces relapse risk by about 39%. Compared with digital alone, combining digital with in-person is the most robust use right now.
Online communities don’t replace in-person treatment. They fill the time between sessions. For the people who can’t stay in treatment, or aren’t getting there in the first place, the meaning of having a first door to open is not small.
What’s in your hand at 10 PM in front of an ATM. That specific question keeps surfacing, downstream of all of these debates.
References
- Suler J. “The online disinhibition effect.” CyberPsychology & Behavior. 2004;7(3):321-326.
- Kelly JF, Humphreys K, Ferri M. “Alcoholics Anonymous and other 12-step programs for alcohol use disorder.” Cochrane Database of Systematic Reviews. 2020;Issue 3:CD012880.
- Christensen DR et al. “Effects of a smartphone-based intervention with reSET-O on opioid use disorder treatment outcomes.” JAMA Network Open. 2021;4(2):e210055.
- Kwan I et al. “How effective are remote and/or digital interventions as part of alcohol and drug treatment and recovery support? A systematic review and meta-analysis.” Addiction. 2025.
You may also like

Recovery Isn't About Going Back
You quit drinking and wait to get back to who you were before. Then one day it hits: the person you wanted to return to was the same person who was about to start drinking. Recovery isn't returning to the past. It's the practice of carrying your flaws and continuing anyway.

People Who Cheered Others On Recovered Better: Surprising Data from an Addiction App
In an addiction recovery app community, the people who wrote comments on others' posts had longer streaks themselves. Even when controlling for app usage, the gap remained. 599 users' worth of data lines up with what 12-step programs have known for nearly a century.

How Self-Blame Sabotages Addiction Recovery, and What Actually Helps
Research shows that self-blame after a relapse doesn't motivate change. It raises cortisol, weakens impulse control, and makes the next relapse more likely. This article covers the neuroscience behind that cycle and practical alternatives like ABC analysis.

Reflection Changes Behavior: What Behavioral Economics Tells Us About Recovery
Dan Ariely's Ten Commandments experiment showed that a brief moment of moral reflection, even when participants couldn't remember what they were reflecting on, nearly eliminated cheating. The same mechanism applies to addiction recovery through implementation intentions and self-compassion.
QuitMate
Together, you can quit
Connect anonymously with others who share your struggle. Whether it's alcohol, smoking, gambling, or other habits, you're not alone.